
I finished the last article I wrote - the one on auto-augmentation - with a segue into this one. Just to recap, I was asked a question by a follower on Instagram that really bundled two different topics together, but I think they are better considered separately. So, this is kinda part 2 of a double-billing. How exciting.
Given that we've covered the auto-augmentation part of the question previously, in this article I want to look at the factors that are associated with shape, and how surgical techniques can be responsible for certain breast shapes (both good or bad!) after procedures like mastopexy or reduction.
So, the second part of the question I was asked was: can we define why some breasts look flat, and square or boxy, after a mastopexy or breast reduction? The thing to really emphasise is that whether a breast looks flat or square has nothing to do with whether an auto-augmentation has been done. Not really. It comes down to how the operation (whether a mastopexy or reduction) is planned, how it is executed, and how a patient heals.
A breast can still look perky, projected and round without an auto-augmentation; but an auto-augmentation can't save a breast from looking square if the other stuff isn't done right.
Now, the picture above shows a more typical breast reduction marking - a larger, heavier breast, with the red area indicating the tissue to be removed. What you can't see here due to the perspective is the lateral "wing" of tissue (on the outer part of the breast) which is also removed.
Why does this matter?
Well, whether we are talking about breast reduction or mastopexy, we can never get away from the "human" element: that is, the person who draws these markings is a human, and the specific pattern of markings depends on the individual qualities of the person having the surgery; the specific way in which the surgery is then done depends very much on the surgeon, and their ability to maintain their bearings when navigating the surprisingly difficult 3D topography of the breast; and the specific way the breast tissues heal and settle over time are completely individual, and are determined by both the surgery performed and the patient's own basic biology.
That isn't my way of making excuses for shitty outcomes, just to be clear.
But let's work through those points to understand how each element can contribute to eventual positive (round, natural), or negative (flat, boxy, weird etc.), outcomes.
Let's start with something that should be obvious, but perhaps isn't.
When a surgeon is marking a patient pre-operatively, there are (or should be) a whole bunch of specific thoughts and ideas that are being applied.
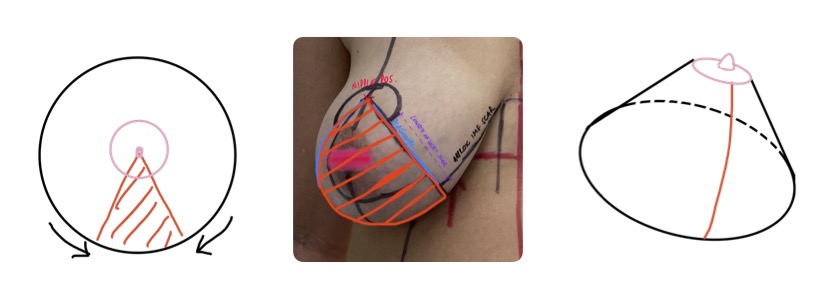
The are 4 major variables in the marking process are: 1) where does the nipple go; 2) what will the specific angle of the diagonals be (ie. how much will the breast be narrowed; 3) how long will the vertical scar be; and 4) where will the inframammary scar end up.

All of these markings are TOTALLY dependent on the surgeon, and all of these markings have the ability to TOTALLY bugger up the result if they are either incorrectly conceived, or there is a slavish commitment to simply cutting on the line without making intra-operative adjustments. It should go without saying that breast reduction cannot ever be a boiler-plate operation where the same lines are drawn on every patient. Every patient, every breast, every body, demands individualised markings to account for proportions and anatomy.
Side note: I see quite a few American surgeons on instagram showing themselves marking breast reduction patients pre-operatively and they are using fixed, wire templates to draw out the nipple and the diagonals (which we'll discuss below). It makes me cringe. As a rule, that is a terrible idea.
Let's start with nipple position. There is a very frustrating idea that remains prevalent in plastic surgery that the nipple MUST be placed at 21 cm from the top of the breastbone (the sternal notch). Where does this number come from? Well, the answer to that is that back in the 1950's, in a characteristically creepy old-white-dude kinda way, a surgeon got 150 "volunteers" (read: healthy young women who, so the story goes, were actually cadets of some description who really didn't have much choice) to whip off their gear and submit themselves to measurement. Of those 150, 20 were deemed "aesthetically perfect" (creepy much?) and thus we were provided with a set of measurements considered to be a universal aesthetic standard of brilliant boobs. In case you're wondering, a measurement of 8.5 inches from the sternal notch or mid-clavicle was the number that mattered.
In the academic paper I am referring to, the following commentary jumps out:
"It will be observed that there is scarcely any difference in the breast dimensions of the normal woman, no matter what her height or weight may be. The conclusion to be drawn, therefore, is that there is a standard type of breast, the measurements of which would be esthetically correct for any woman." (Penn, Br J Plast Surg, 1955)
Wow. Surgeons in the 50's were wild, huh? I think we can consign this thought to the bin-fire of historical thinking. The concept of an "aesthetic standard" that can be applied across all body types/shapes/sizes etc. is patently absurd.
And yet, like I said, the idea sticks, and junior surgeons to this day are taught to simply measure 21cm from the sternal notch and ta-da *surgeon does jazz hands*...there goes the nipple.
And now, having thrown some serious shade at the idea, allow me to explain my approach to this element of planning. Also, just to be clear, I am not necessarily offering a unique perspective here - many surgeons will be using similar concepts and techniques.
First off, my ranting and raving above is not to say that 21cm is always wrong. It is, more specifically, to say that 21cm is often wrong, and only sometimes right. Clearly, that then raises the question of what is the correct measurement, and indeed whether we should be measuring at all.
What is the value of a measurement? Good question. If we can cast aside the premise that a single universal standard can be applied to all bodies, we might then consider perhaps a measurement range. But that is only useful if we can also determine where, within a given range, a certain patient's nipple should sit. You can see that measurement alone is not the answer here - we need more information.
We also need to reframe the question. What we need to know isn't where to mark the nipple pre-operatively (although that is important to consider, obviously). What we really need to know is where will the breast volume end up after an operation is performed. Because it is only by knowing where the breast is going to end up that we can determine nipple position. Why? Because the nipple position should end up being centrally located on the eventual breast mound that is to be created. The nipple should ideally sit at the most projected point of the breast, with a slight upwards tilt to the areola perhaps. That is the important information in all of this, and it is only by understanding that goal that a surgeon can start to figure out how to mark the intended nipple position for a given patient.
...the nipple position should end up being centrally located on the eventual breast 'mound' that is to be created...it is only by understanding that goal that a surgeon can start to figure out how to mark the intended nipple position for a given patient.
Which means we need to understand the anatomical and patient variables that influence the final breast position.
It also means a patient needs to understand why they won't necessarily be able to achieve a "high-breasted", "perky" breast if their anatomy won't allow it. Of critical importance, a patient also needs to understand therefore why a high nipple position is not something that will automatically lead to a high breast position! Or, to put that another way, the goal of any breast reduction or lifting procedure is NOT to put the nipple as high as it can go...because that totally disregards the fact that unless the breast volume can also be positioned high on the chest, the nipple will simply end up too high for the breast, which results in something referred to as superior nipple malposition, which manifests as a particular outcome that no patient will ever appreciate: nipples that pop out of the top of a bra or swimsuit (not cool).
...the goal of any breast reduction or lifting procedure is NOT to put the nipple as high as it can go...unless the breast volume can also be positioned high on the chest, the nipple will simply end up too high for the breast, which results in...a particular outcome that no patient will ever appreciate: nipples that pop out of the top of a bra or swimsuit...
Now, the anatomical variables I referred to above can really be boiled down to the level of the breast crease (for most patients, with some consideration given to things like patient height, shoulder width, chest:abdomen ratio, and overall body proportions). What I mean by that is that for a patient with a naturally high breast crease, when we reduce or lift a ptotic/drooping breast, we can expect that the breast can be elevated into a higher position as determine by the breast crease; on the other hand, if we were to try to lift a breast with a naturally low breast crease up to a similar level, with a similarly high nipple position, then that second patient would end up with superior nipple malposition, and a breast that would look "bottomed out".
So, we have to look at the patient as a whole, and then we will find ourselves marking a nipple anywhere from 19cm (for a petite woman with a naturally high crease, for example) to perhaps 24cm (for a taller woman with a naturally low breast crease).
But let's also come back to the question of whether we should be measuring at all. And here, my thoughts are that measurement is mostly of value as a way of confirming symmetry, from right side to left side. But a slavish adherence to a certain number when marking the nipple is generally speaking, not helpful.
"...measurement is mostly of value as a way of confirming symmetry, from right side to left side."
One final point to make here is to refer to something of a cheat code that I like to use in two particular scenarios: cosmetic auto-augmentation mastopexy, and explant-mastopexy. That cheat code, which ensures more flexibility in positioning the nipple, is to only mark the nipple position once the breast has been shaped and positioned. This technique (which, again, I think many surgeons employ), means that the nipple can be properly positioned relative to the breast shape and volume near the end of the case, and with the patient in a seated position. When we do this (and as many of my patients will know), the nipple position still has to account for the expected post-operative changes that will occur with time, namely expansion and softening of the lower pole (see below). When this cheat-code is used, there still needs to be some approximation of the intended nipple position to allow the marking of the diagonals (see below), but the circular areolar incision is not marked in.
It is worth saying then, that no matter how the nipple position is determined, what we should see early in the post-operative period is a nipple/areola that actually tilts DOWNWARDS, such that over time, with the expansion of the lower pole, the areola progressively shifts its attitude from a downward tilt, to a forward facing position, and eventually to a subtle upward tilt. This is a common part of the discussion I have with my patients at the 6 week review post-op, because at this time most patients will still have a downward tilt that won't resolve until around the 4 month review.
Righto, so now we have the nipple position marked, this allows the next step, because the nipple position forms the apex of a triangle that is instrumental in the shaping of a breast.
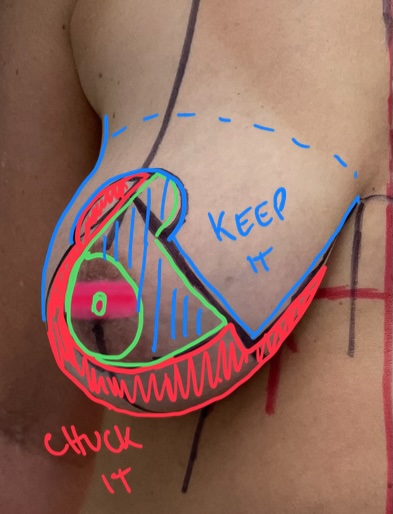
The basic concept here is simple, and something that primary school kids can understand: take a circle of paper, cut out a triangle, and then put it together. What you make is a "cone". Now, clearly, the breast is not a flat piece of paper, but you can probably visualise what we are trying to achieve here. But removing a certain amount of tissue (which, when marked on the surface looks like a triangle, with the new nipple position at the apex), and then putting things back together, we are effectively "coning" the breast to create projection, narrow the breast base, and control the shape of the breast. This effect is one of the major attractions of the superior and superomedial pedicle techniques, but the same effect is totally absent for surgeons who use inferior pedicle techniques. So this is both a marking feature, but also a conceptual/technical feature which has lead to many surgeons abandoning the inferior pedicle techniques.
This actually is one of the answers to the original question posed in this article - the inferior pedicle is a technical choice that is classically associated with a breast that looks flat, and square, precisely due to the lack of "coning" that is possible with that technique. The inferior pedicle is also prone to bottoming out due to a lack of control of the lower pole.
Anyway, the diagonals diverge from each other at an angle, right? But what angle? Is there a right answer.
Again, not really. It depends on the patient.
The idea of how that angle is determined is more important than the angle itself. And this requires a combination of a specific manoeuvre, experience, and the ability to understand the longer term impact of how the breast can be manipulated.
So, women who have had a breast reduction will be familiar with what I am about to describe.
When a surgeon is figuring out the diagonals, on each side they will manipulate the breast, pushing the tissues both outwards (to mark the inner diagonal) and inwards towards the cleavage (to mark the outer diagonal). What the surgeon is attempting to do here is to mimic the effect of removing that triangle of tissue between the diagonals and the narrowing effect it will have on the breast, as well as how that effects the shaping of the breast. By pushing more or less, they can mimic the removal of more or less tissue. With the breast held in a certain position to shape both the inner and outer aspects, a vertical line (a plumb-line if you will) that drops from the planned nipple position, can then be drawn which, when the breast is released, will spring back into a diagonal. Do that twice for each breast, and we have our diagonals sorted.
Clearly we would want a similar effect to be created on both sides, so there need to be checks for symmetry. Also, we have to have a particular care for marking the diagonal on the outer aspect of the breast, because this one will be more important in determining the narrowing effect - if that outer diagonal is marked too aggressively, this can lead to a breast becoming overlying narrowed (especially in mastopexy cases), which then exposes the chest wall in a way that is rather unaesthetic. You'll see that effect a bit on social media and it is a hallmark of what I would consider overly-aggressive surgery for ladies having a mastopexy or a small volume reduction.
The length of the vertical scar is not an accident, or just something that happens. Despite what some surgeons will assert (especially those who have faith in "lollipop" scar techniques), I don't believe that the infra-mammary crease will just magically "find it's own level" either.
The length of the vertical scar is a distinct choice which must be made by the surgeon, and it is fundamentally tied to the the desired position of the IMF, as well as the decision about nipple position.
Let me explain.
We often talk about the need, in breast surgery, to create a stable "shelf" under the breast, which then supports the breast in a given (often higher) position. This "shelf" is created by reinforcing or reconstructing the breast crease. Which is what many surgeons are actually talking about when they utter those magical words: internal bra.
The shelf effect is then reinforced by stitching together the breast "pillars" (the edges of the breast tissue that remains after the lower pole "triangle" has been removed). The pillars can be thought of as the internal aspect of the diagonals that were marked on the skin surface.
What I then go on to say is that we need to build upwards from the crease. So, working along those lines, we can then deduce that we need to treat the breast crease as the foundation, with the vertical scar/pillars representing, simply, the desired distance from the breast crease to the areola, and this distance has to account for things like breast size, patient height etc.
So we need to make a decision about where the vertical scar starts (ie. where the bottom of the areola is positioned) and where it ends (ie. where the incision is marked for what will become the breast crease).
Depending on whether we have already marked and cut out the new areolar border, there is some variability. If we have taken the approach of only marking the nipple position once the breast mound has been formed (for mastopexy and explant-mastopexy cases), we can then determine the length of the vertical scar by measuring upwards from the crease to mark the lower edge of the new areola.
It's a little different for a breast reduction where a surgeon has already committed to a nipple position - in that case, I then work in reverse, with the vertical scar length having to be carefully matched to the idealised position of the breast crease incision, based on where we have placed the nipple. The flexibility in the breast reduction being that we can remove more or less tissue to allow us to ensure that the incision matches the new crease position; in a mastopexy or explant-mastopexy, the goal is not to remove tissue, so we need to think differently and place the nipple correctly relative to the crease and breast.
That one is tricky to describe because it is the one with the most wriggle-room. Modification of the vertical scar length intra-operatively (regardless of which procedure we are doing) is something that demands experience. I think I've gotten better over time in that respect.
Righto, that takes us neatly into the next section, which is how do we determine where the incisions should be made to allow that IMF scar to sit correctly.
This is an interesting one for me because I think I probably do this a bit differently to most surgeons, and that is just a consequence of something I stumbled across years ago which I felt allowed me to get better results.
So, especially when surgeons use a T-scar for their breast reductions or mastopexies, most surgeons will simply mark the position of the planned IMF incision on the breast based on the predetermined nipple position: in other words, they draw in the areolar border, then they measure down for their vertical scar length along the diagonals, and then they draw in an IMF incision across the breast from there. Now, that can work, but in my opinion, there is a very high chance that the marked incision doesn't quite result in a clean contour (possibly resulting in a square shape), or will leave dog ears.
My preference is actually to (a bit like with the nipple position in many cases) only mark the IMF incision part way through the surgery. The way that works is that I remove the breast tissue between the marked diagonals, and then I only figure out the IMF incision after I have stitched the breast tissue (the 'pillars' I mentioned in the previous section) together - in other words, I cut the wedge out of the circle and then make the cone first (as described above). What this does is it actually forces a NEW breast crease to reveal itself on the surface of the breast at this stage, and for me that determines the placement of an incision that is far less likely to result in contour problems or dog-ears.
Of course, the position of the IMF scar also implies some discussion about "dog ears". But perhaps that is for another time. Suffice it to say, I think dog ears are largely avoidable. Yes, in some cases we don't get it quite right. In some cases patients will be perfect early on but then there seems to be some degree of dog ear formation over time, perhaps with weight fluctuation or just with settling. But mostly, i think dog ears can be prevented.
So clearly, markings are super important in creating a round, well shaped breast with mastopexy and breast reduction procedures. Those markings have quite a bit of overlap with execution for me, given that I make a lot of intra-operative determinations.
There is more to execution though.
Procedures like a mastopexy are not just "cut-on-the-lines" operations.
The breast remains a 3 dimensional structure, and there is substantial shift in the tissues based on posture. That has to be factored in. What we mark (when a patient is standing up) starts to look very different when lying down. The surgeon has to be able to appreciate how an operation done on a supine patient translates into an upright patient. If a surgeon does just cut on the lines, then that only accounts for what happens at the surface; it doesn't account for what happens within the breast tissue itself.
I think the easiest way to explain myself here is with three key examples.
The first example is all about "thickness".
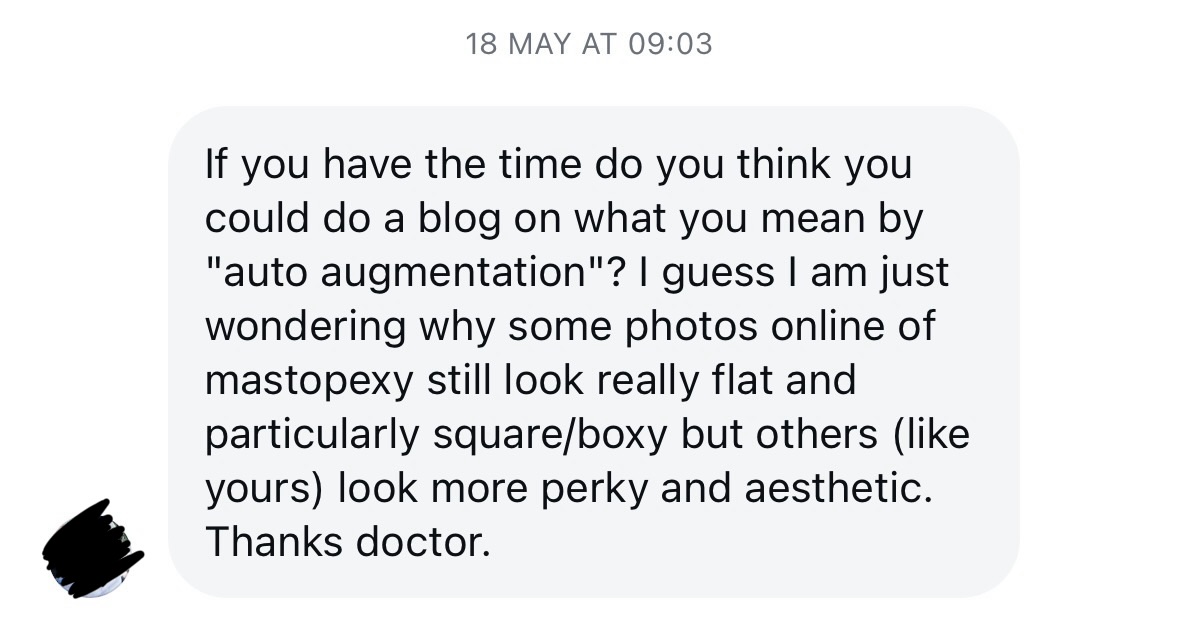
Take this (now clumsily coloured) image that we've considered previously. It is often said that breast reduction is more about what you keep than it is about what you remove. In this image, the greens(ish) shading indicates (in a standing patient) the tissue to be removed full-thickness (that is to say, we remove the tissue from the skin, right down onto the chest muscles in a block. The reddish shaded areas are those parts of the breast that we are keeping in order to rebuild a new breast shape. However, we have the option to thin out those red areas.
It is often said that breast reduction is more about what you keep than it is about what you remove.
Now, if we go back to the "coning" concept I mentioned above, then we can think about thinning out the tissue we have kept as a way of reducing the projection of the breast.
So the more we thin the remaining tissues out, the smaller the breast can become. And this is really important to understand I think: the nipple position is NOT a factor in determining breast size. Higher does NOT mean smaller! The markings on the skin are determined by the patient's anatomy which has more to do with proportion, and avoiding aesthetic distortion of the breast relative to the chest wall. The final (cup) size of the breast is then determined by how much projection we remove by thinning the remaining tissues.
The nipple position is NOT a factor in determining breast size. Higher (nipples) does NOT mean smaller breasts! The final (cup) size of the breast is determined by how much projection we remove by thinning the remaining tissues.
This concept is one that doesn't get taught to training surgeons, and I think putting it in those terms is useful for both surgeon and patient alike.
Having said all that, there is a limit. Because the blood supply to the remaining tissues of the breast - and, critically, the nipple - must be protected in breast surgery, if a surgeon thins out the tissues too aggressively, this can (and will) compromise the blood supply to what we are keeping.
So when you hear those horror stories about "dead" nipples, unfortunately that arises due to overly aggressive thinning of the tissue under the nipple, which borks the blood supply. This means that there is a lower limit to breast size. And it also helps people to understand why, if we are interested in mitigating risk of complications, we have to be very cautious about over-reducing a breast. If someone presents with a G/H/I/J cup breast and wants to be a B cup, that just might not be possible without causing blood supply issues.
The second example I'll use here relates to the inframammary fold.
It should be emphasised that the inframammary fold is actually a pretty clear anatomical structure in most patients - there is a layer of fibrous tissue that actually anchors the position of the fold (at the skin level) to the deeper chest wall structures. It should also be emphasised that the direction of that fibrous tissue is not straight inwards - the anchoring fibres run at an angle upwards as they course deeper towards the chest wall.
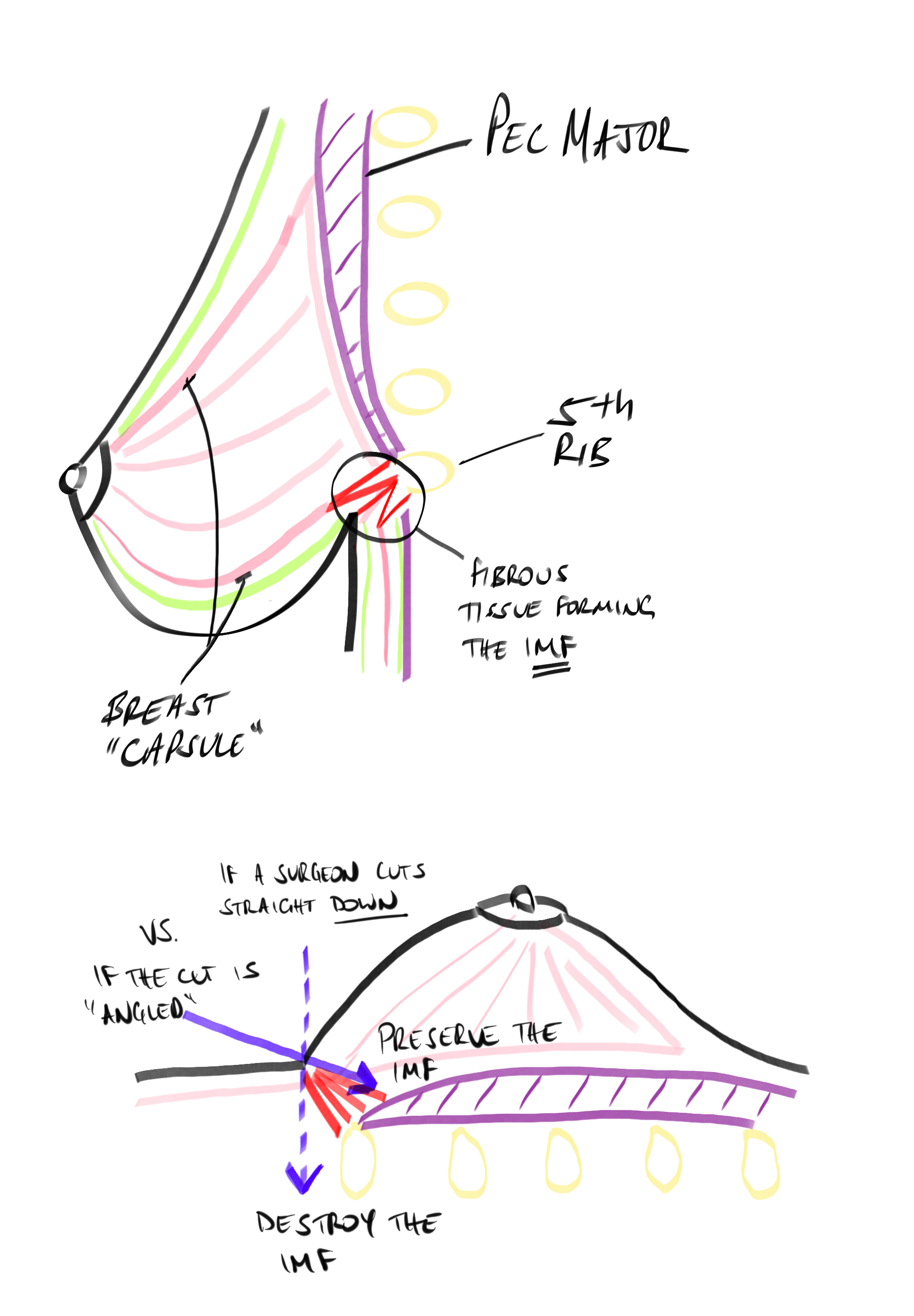
To paint this picture, let's use the diagram above here. The inframammary fold is formed by a "ligament" (the fibrous tissue) of sorts, which is shown in RED, attaching deep onto the chest wall around the level of the 5th rib (and approximating the level of the attachment of the Pec muscle). This ligament tethers the skin and subcutaneous tissue in most women, creating the natural crease.
Yes, some ladies lack this structure naturally. But for the sake of argument, let's accept that all breast have some version of this structure.
The more relevant part of this diagram is the lower image which shows the same breast once the patient is lying down. This is the position the patient is in during surgery.
Now the key is how the surgeon makes an incision and cuts through the tissues in the existing inframammary crease during surgery: do they cut straight downwards towards the chest wall, or do they angle the cut quite significantly upwards towards the head?
What I'm showing here is that if the cut passes straight down to the underlying ribs, then the incision will divide or pass below the ligamentous structure forming the IMF. This results in a total loss of control of the crease, which is a disaster for most breast procedures.
On the other hand, if the cut is angled towards the head, then the surgeon can skim along on top of the ligament, allowing the removal of the lower breast tissues whilst preserving the ligament and therefore, preserving the natural crease structure.
Why is that important?
As I discussed above, when it comes to breast shape, the breast crease plays a massively important role. If the crease acts as intended, it acts as something of a hammock for the breast tissue it supports. If the breast crease ligament has been destroyed (and not deliberately rebuilt) then this may be one of the reasons that the crease can drop, and this may be associated with a square breast shape when looking from the front.
And the last example I'll give you is how the direction of the breast crease scar relates to the outer breast curve.
This last one is (if I'm honest) one that a) took me a while to figure out and b) I still tinker with, and if I'm honest there are times when I don't get it as perfect as I want.
Whilst we have long since moved away from the idea that we can shape the breast by shaping the skin (we can only properly shape the breast by shaping the deeper tissues, and then the skin is simply allowed to drape over the top of that), there is one part of the surgery where we do rely more on the skin for shaping, and that is the outer or lateral part of the breast.
So, very commonly when you are looking at breast reductions online, you'll often see something which I was guilty of as well until perhaps 4 or 5 years ago: the breast crease scar continues running horizontally beyond the lateral edge of the breast, and around the side of the chest wall. Now, this happens because the surgeon assumes that the scar has to run in the line of the old breast crease, which often continues into a bit of a skin crease on the side of the chest for those ladies with a heavier bust and a little more fullness under the arm.
If the scar just runs horizontally out towards the lateral chest wall, this can contributes to that squareness that is sometimes seen after a breast reduction and mastopexy.
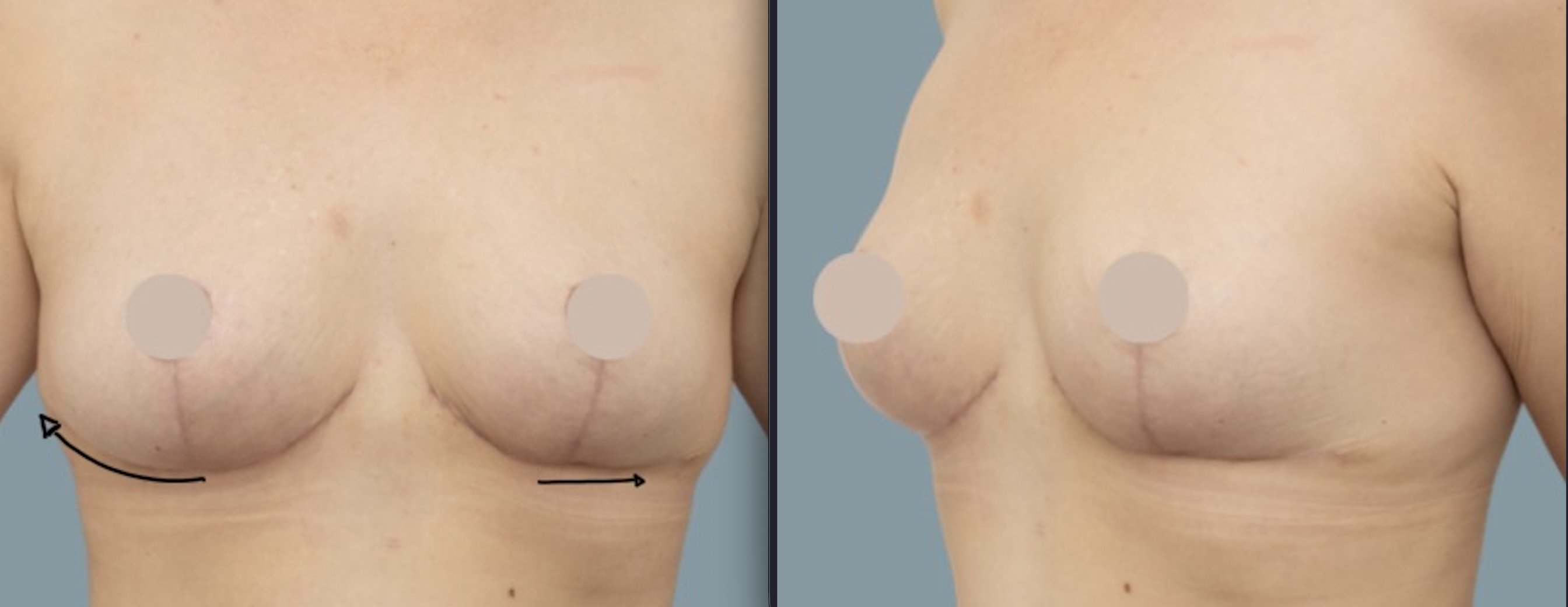
In reality, the scar direction needs to change to match the future shape of the new breast crease once the breast is smaller - this means a narrower breast, and tighter curve, and the scar needs to change direction and run out of the old breast crease and angle upwards somewhat to mirror that new breast curve.
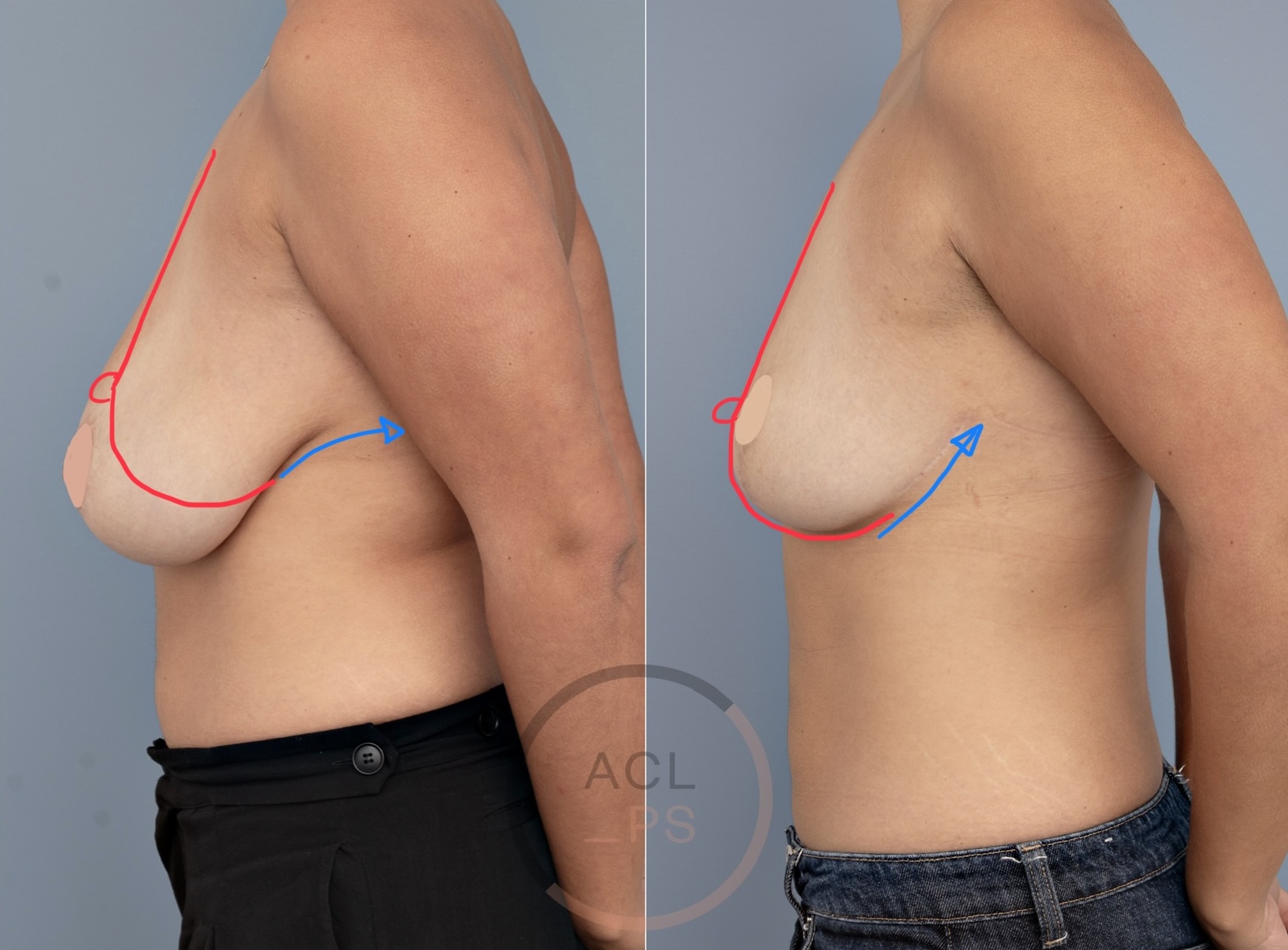
There is also (quite) a bit of internal stuff that I do (I presume others do something similar, but I'm not really sure because this is one of those things that isn't really discussed or described in texts) which involves grabbing the fascia on the side of the chest and dragging it forwards internally and hitching it onto the chest wall. This is what mimics the action of a patient who uses their hand to pull the breast forwards and around towards the centre of the chest - the effect of that action is to create a smoothing contour effect on the side of the chest wall, where there was some fullness there to start with (in association with a heavier bust). Useful little manoeuvre I think.
Many surgeons will also use liposuction as a shaping tool but in my experience, if that scar direction isn't correction, the liposuction struggles to prevent that squareness on its own.
Ok, we're getting there.
The last element to consider is the one that can be a little random, which may depend a little on luck (because intrinsic patient factors play a role), but can very much be influenced by the post-operative recovery process. This is the one that makes me turn into a bit of a dictator post-op: if patients do the wrong thing here, they can be responsible for an increased risk of complications. But of course, there is stuff that a surgeon can do to make it worse as well.
I think the intrinsic patient factors that play the biggest role in the settling process have to do with tissue quality questions. What we really mean here is how resilient the breast tissues are going to be, how elastic they are and how well the tissues can support the breast weight post-operatively. And these factors then play into one very specific aspect of the settling process: lower pole expansion.
No matter which surgeon does it or which patient has it, a breast reduction (or a mastopexy) is not "stable" until around 6 months post-op because in that first 6 months, the lower pole continues to expand. Which means that the surgeon needs to expect it and accommodate it in the surgical plan. But the challenge rests on figuring out how much expansion any given patient will experience.
What we see is that for patients with very large breasts or very stretched tissues, the intrinsic ability of the tissues to then support the higher, tighter breast shape created in surgery is not going to be the same as a lady who needs a more modest reduction, who has a denser breast. This then represents the luck part of the equation for the patient.
So, the biggest way in which I think surgeons can influence the settling process is really based on some of the decisions they make, and which have been discussed above. If the decisions about certain measurements, scar positions etc. are not right, then the settling process will be compromised. The other thing that really matters here is closure technique and perhaps choices regarding dressings. If surgeons use the wrong suture type, if the placement of those sutures isn't right (at various different points and in different layers), and if the wounds aren't supported post-op (with certain dressings) then this can all influence the settling process, leading to problems like bottoming out or a boxy shape, and it may mean that patients are more likely to experience stuff like suture "spitting", which may then lead to worse scars.
It is also important to point out that the settling process is rather different if we compare the technique that I use (a superomedial nipple pedicle, with an "anchor" scar) versus an inferior pedicle technique with an anchor scar (which will tend to bottom out and look square), versus the techniques using so-called "lollipop" scars (which, in my experience, create a substantial lower pole distortion which is revealed when the arms are elevated).
Now, the bit that I then put back on my patients has to do with compliance with post-op instructions.
I think it fair to say that the 6 week healing period can be a little challenging for patients. We do ask a bit of them: sleep on your back, don't be too active, control what you are doing with your arms ("T-Rex" restrictions, anyone?). But there are (of course) good reasons for all of it.
I think this can really be boiled down to two concepts: minimising swelling/oedema, and preventing seromas/fluid collections. The basic premise here is by doing the right thing, your risk of complications is kept low; if you decide to go hiking, or to play golf, or some similarly silly thing, then you are putting yourself (and your outcome) at risk. Typically, self-interest is a solid motivator here...but not always.
I've tried to offer some insight into how surgeons (should) think about breast shaping. If you take only one thing away after reading this, I want to emphasise that any breast reshaping procedure (mastopexy, reduction, explant procedures, tuberous breast corrections, asymmetry corrections, reconstructions - any of them!) relies heavily on the surgeon and just as heavily on intrinsic patient factors that may be out of our control.
These are the burdens we take on ourselves as surgeons, but we must also accept that we are only human. Not every outcome is perfect, and that is to be expected. So whilst both surgeon and patient alike may hope for perfection, we must be willing to accept that perfection is typically an unobtainable goal.


