
The endless sales pitch from plastic surgeons becomes rather tiresome I suspect. The shameless social media activity, the desperate attempts to stand out amongst a crowded field of peers, writing dodgy blog articles to win the SEO race (lol)...
It is inevitably true then that as surgeons seek to commoditise their expertise and experience, that they find efficient ways to abbreviate technical concepts into sellable labels.
"Auto-augmentation" is a clear example of this. It also doesn't hurt that it looks like something it isn't, with enough plausible deniability to pretend that no-one really meant that anway!
Anyhoo, this article was prompted by a recent DM on instagram. I suspect I was being contrary in some fashion or another, and someone asked me:
And so, because I am nothing if not a slave to the churn of SEO, desperate to float to the top of the AI slop pile, here we go.
Auto-augmentation is a convenient short hand that gives an impression of something far greater.
But first things first: auto-augmentation is not a breast enlargement in any sense of the term. But that also depends a little on perspective.
The best thing to do is to take a step back, and first let's consider mastopexy procedures (because that will help make more sense of what we're talking about).
In the "traditional" sense (ie. how most surgeons do it), a mastopexy is just a small breast reduction. Because every breast reduction also elevates/lifts the breast (ie. every breast reduction is also a mastopexy), for many surgeons, they view mastopexy as being an operation done for ladies with a little excess breast volume, in whom the repositioning of the breast is facilitated by removing some of the breast tissue at the bottom of the breast.
Now, to be fair, that isn't always a bad solution. For some ladies, a small reduction is actually the right operation.
But the point I would make is that a small reduction is still a reduction.
A mastopexy is (and should be) something different.
I think that a mastopexy is an operation in which the entirety (or at least the vast majority) of the breast volume should be preserved. In other words, it is an operation for someone who wants/needs ALL of their volume, just in a different position on the chest. I think this is important because it creates the fundamental distinction between a reduction and a mastopexy.
So just for total clarity: every breast reduction also entails a mastopexy, with elevation of the breast; but in my hands, a true mastopexy never includes reduction of the breast volume.
So, if we use that definition of a mastopexy, we then have to ask the question: what happens to the breast tissue in a mastopexy to allow the breast volume to be repositioned.
Which then brings us to auto-augmentation. And I should add that, for me, every mastopexy involves an auto-augmentation.
In reality, auto-augmentation is a flexible concept, and it isn't just limited to pure mastopexy procedures. The concept can be equally applied to breast reduction style procedures - for example, we might selectively preserve a certain part of the breast volume with a particular purpose (very commonly, this is how I approach tuberous breast correction), whilst resecting another part of the breast volume that does NOT serve a purpose. But let's assume that the goal in every case is the maximal preservation of breast volume.
It is hard to fully separate the concepts of mastopexy and breast reduction, simply because there is a lot of overlap. And for me, it is the overlap that really helps us define auto-augmentation.
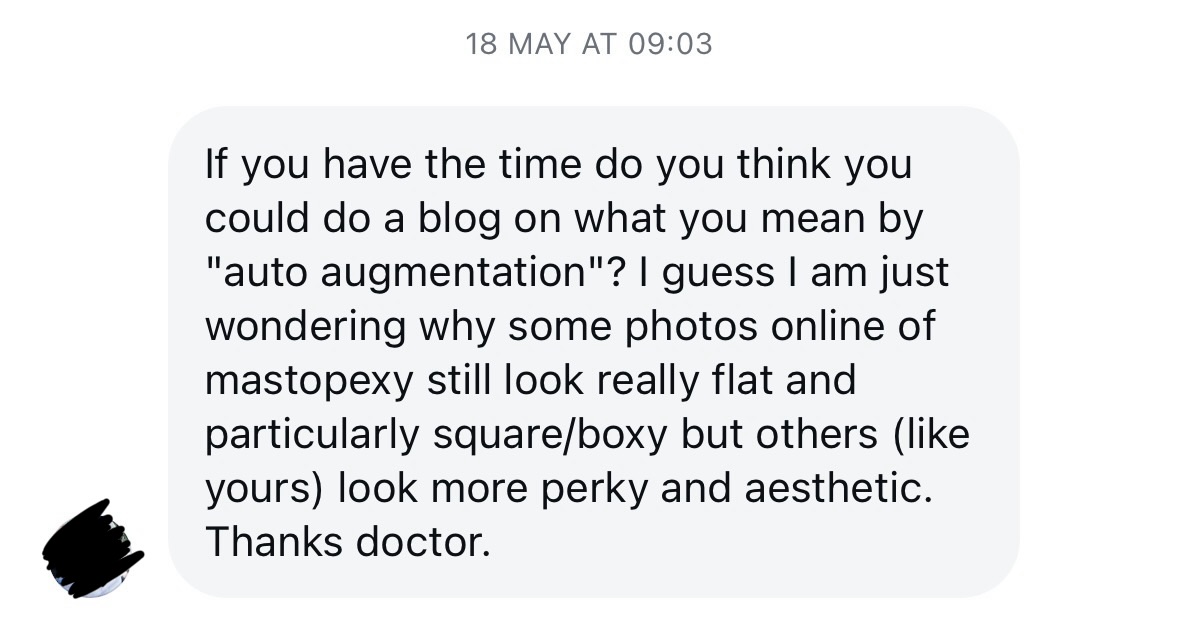
So, take the picture above: we can look at this from both the perspective of mastopexy as well as breast reduction, to help understand the differences.
The focus here is on the lower part of the breast - you can see both a green outlined area as well as a purple one. The green outline includes all of the tissue at the bottom of the breast that would be removed in a traditional breast reduction or indeed, in a traditional mastopexy. If that green tissue is removed, then the differentiation between a breast reduction and a traditional mastopexy is mostly a question of degree - if the breast starts off large/heavy, then the green area represents a much more significant volume of tissue below the breast crease, and this would then be consistent with a breast reduction; if the breast is small/deflated, then the green area is representative of a rather sparse amount of tissue, and its removal is simply to facilitate the lifting movement involved in a traditional mastopexy.
But what if we didn't just remove that tissue?
There are two typical options we look at here.
On the one hand, we could try to preserve the entirety of the green area in the image above - this is precisely what I do for patients having a mastopexy who have either experienced significant weight loss (eg. after bariatric surgery, or more recently with GLP1 agonists), or those ladies having explant procedures.
Or, on the other hand, we could choose to preserve just a central portion of that green area, as indicated by the purple outline (sometimes in conjunction with the medial "wing" of the green shaded area towards the cleavage), which is more typical of a mastopexy performed for a lady with ptosis (droop) but without significant deflation (ie. those ladies with firm, full breasts, albeit breasts that are sitting lower than they would like).
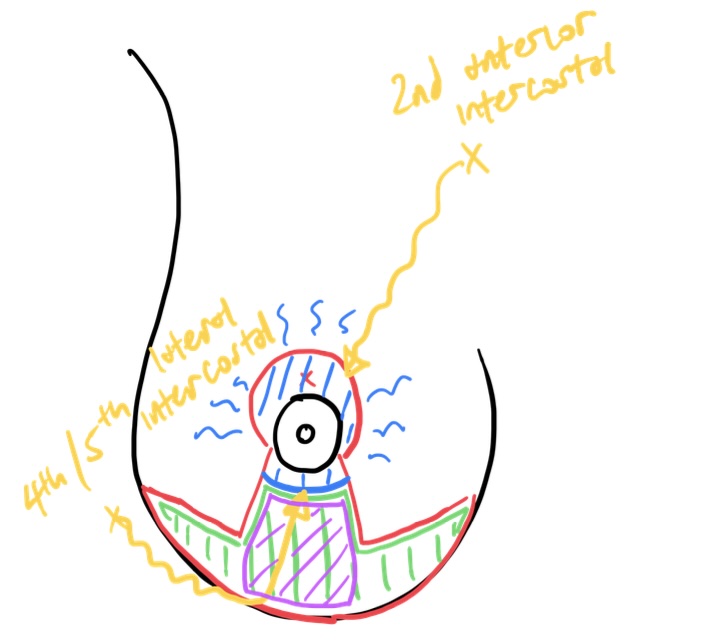
In either case, the preserved tissue can be a) shaped, b) mobilised/moved, and c) fixed in a new location, buried inside the breast (after the skin layer of the auto-augmentation tissue is simply peeled off). It is this action of burying the tissue and fixing it to the underlying chest muscles that really gives the movement its oomph, and leads to the "auto-augmentation" label. If we position the tissue higher in the breast, with more volume behind the nipple, this has the action of subtly increasing the projection of the breast. So, once the mastopexy is completed, the breast sits high, AND appears to have a bit more projection. So whilst it may not have any additional volume, the breast shape lends it self to the bust looking slightly fuller. Hence, we talk of auto-augmentation - that is, using one's own tissue to enhance the breast.
...the preserved tissue can be a) shaped, b) moved, and c) fixed in a new location, buried inside the breast...It is this action of burying the tissue and fixing it to the underlying chest muscles that really gives the movement its oomph, and leads to the "auto-augmentation" label.
Another rather useful aspect of this process is that the movement of that tissue isn't only straight upwards. We can also shift the tissue towards the cleavage if we need to (as in cases of tuberous or constricted breasts). And of course, we can combine auto-augmentation with fat transfer if we actually want to make the breast larger.


The words used here are important too. When we talk of projection (the degree to which the breast sits forward from the chest), this is typically what people interpret as "perkiness" (to go back to the original DM question).
So that gives you an idea of how I approach a typical auto-augmentation procedure.
Having said that, I should also say that there are some variants that you may come across in auto-augmentation technique. Some I use, some I definitely don't. More on that below.
Thus far, I have really been talking about pure mastopexy procedures (or variants of) as a primary correction. The other application of auto-augmentation that plays a massive role in my practice is for explant procedures, and this is a little bit different to what we've spoken about above. It's also an application of the concept that many other surgeons would not agree with - the majority perhaps would tell you that they way I use auto-augmentation techniques "can't be done". Well, after maybe 5 or 6 hundred explants, I reckon I can speak with some authority to tell you that it does work.
There are very specific considerations for auto-augmentation at the time of explant surgery. There are two important distinctions between this and a standard auto-augmentation, even though the tissue template we use is essentially the same.
Firstly, the usual blood supply to the tissue we use for auto-augmentation in a pure mastopexy normally comes from the chest wall, up through the breast. When someone has previously gone in there and placed a breast implant, that blood supply has been destroyed.
Secondly, the placement of a breast implant most commonly involves incisions made in the breast crease, and traditional teaching would suggest that once there is a scar in the breast crease, we cannot rely on blood supply to come up from the crease into the breast because of that scar.
Now, whilst we cannot change that first fact, we can argue that the second "fact" is actually not true.
In much the same way that we can (typically) move a nipple safely a second time for something like a breast reduction after an earlier breast reduction (with scars around the nipple), we can actually rely on the blood supply over a scar in the breast crease to keep the auto-augmentation tissue alive at the time of an explant. I really must get around to writing that up, because to to the best of my knowledge, it isn't properly described in the literature. Anyway, shall do that when I have time.
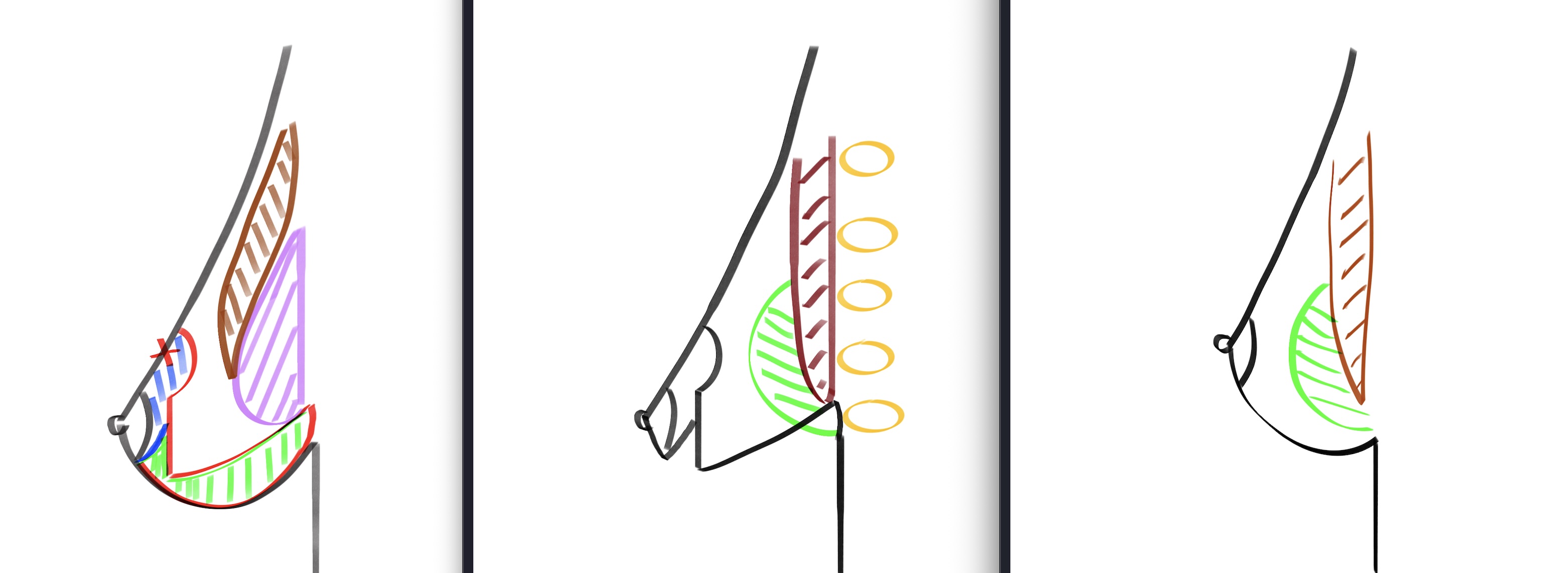
Here is how auto-augmentation works after an explant:
If you take those concepts, in a real patient it looks a bit like this (and yes, I am trying to obscure the gory bits):
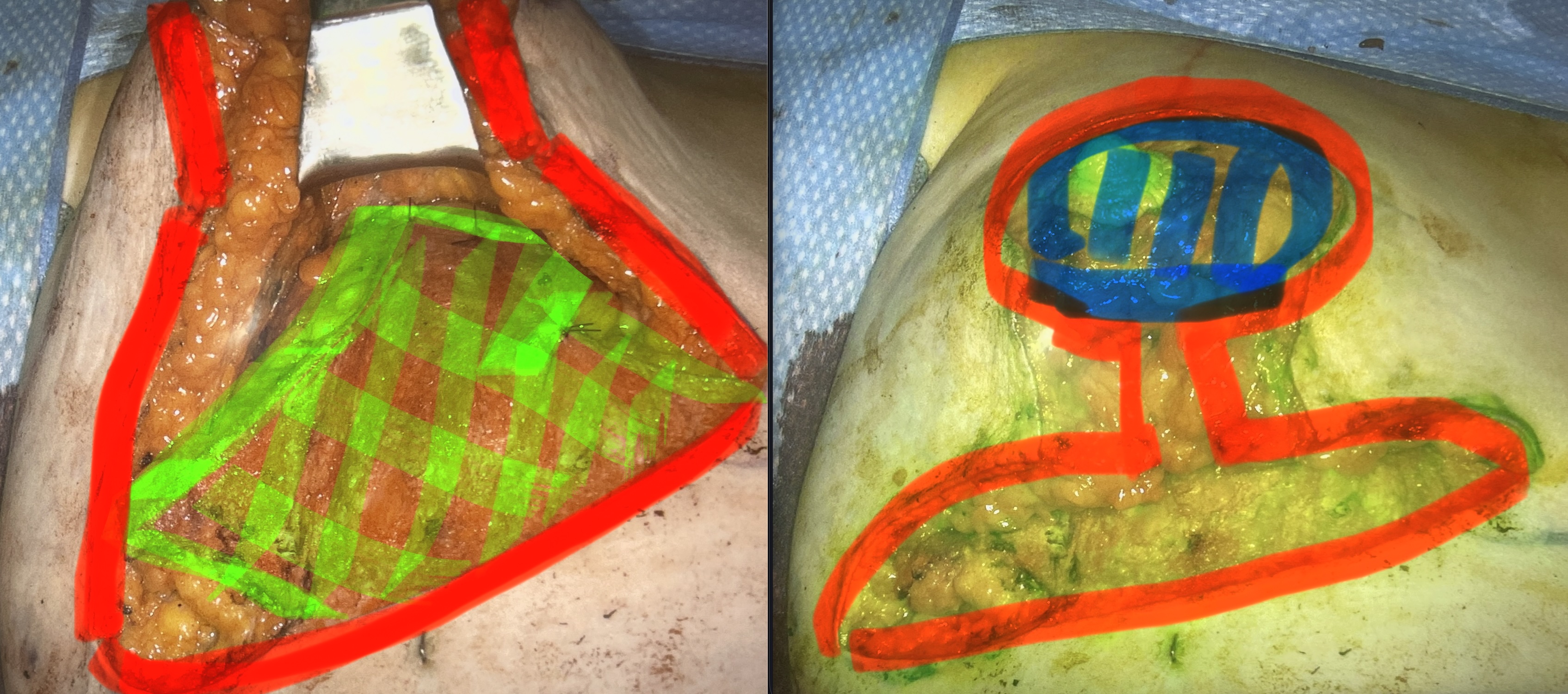
So, somewhat contrary to the "accepted" wisdom of plastic surgeons, we can indeed perform this sort of auto-augmentation regardless of the previous breast implant placement, and generally regardless of scars (even when there is a T-scar from a previous augmentation mastopexy!).
There are, of course, caveats to my statement above about blood supply to the auto-augmentation tissue in explant. In certain cases where that has been a previous breast reduction or mastopexy with anchor/T-scars, the tissues at the breast crease are extremely thin. Whether due to attenuation over time, complications with the original surgery, or repeated prior procedures, if that tissue at the crease is very thin, I don't trust the blood supply in the same way and so I need an alternative.
My preferred alternative in those cases is to actually leave the tissue attached on the breast laterally (rather than inferiorly). This involves a different sort of tissue rearrangement, and I don't think it works as well, but it is the next best option in my opinion when the tissues at the breast fold level are extremely thin.
There are other alternatives too, but I don't like them and I don't use them.
What many surgeons do (and probably the most commonly described technique in the literature) is they keep just the "purple" portion of the lower pole tissues (the central area marked in the auto-aug template at the start of this article) and discard the rest. They keep that central tissue attached to the bottom of the nipple and then they flip it inwards.
This technique (which I think is a terrible technique) causes some common problems: it leads to a substantial amount of tissue loss (which is a big deal if there isn't much natural tissue to start with) and more importantly, it is associated with a specific deformity that I see in ladies who have it done, with a somewhat concave appearance of the lower breast (which happens for a few reasons including underfilling of the lower pole and tension being applied to the bottom of the nipple inset).
I'll finish up this article by saying that this concept of "auto-augmentation" has both its proponents (like your's truly here) and its naysayers. What I find rather interesting is that the naysayers typically rely on silly semantic arguments to justify their opposition. Let me explain that briefly.
So, for those surgeons who are what we might call opposed to auto-augmentation, their opposition rests on the fact that the procedure was, without a doubt, oversold in the past (and perhaps continues to be) when some of the principles were being developed 20-30 years ago. Let's put that down to the fact that the original descriptions come from a different era replete with all sorts of hyperbolic claims being made in the literature.
We should accept that no matter what we do with a tissue-based rearrangement, as in an auto-augmentation procedure, we cannot increase the upper pole volume without the use of a breast implant. Sorry, that is just the way it is. Accept it.
Now, the opponents of auto-aug will then say, "auto-augmentation isn't real" because at some stage, some overly excitable proponent of the technique made an ill-advised claim that they could increase the upper pole of the breast using tissue rearrangement. *Sigh*. I mean, yeah, I get it, on that basis, some of the claims made about auto-augmentation were wrong. Buuuut, that doesn't mean the technique doesn't work.
My counter-argument to the naysayers is this:
Auto-augmentation isn't about the upper pole. It is about optimising the breast from around the level of the nipple downwards. It is about preserving volume whilst still stably repositioning the breast. And it is about projection.
Also, I think (as with a lot of things in plastic surgery), the loudest voices decrying the use of auto-augmentation techniques are those surgeons who just couldn't make the technique work for themselves and got bad results. So, of course, they blame the technique, rather than blaming themselves.
But on to the other part of the question I was asked: can we define why some breasts look flat, and square or boxy, after a mastopexy or breast reduction? The thing to really emphasise is that whether a breast looks flat or square has nothing to do with whether an auto-augmentation has been done. Not really. It comes down how the operation is planned, how it is executed, and how a patient heals. And I think that discussion will muddy the waters a bit if we try to wrap it up with this discussion on auto-augmentation. So, I'll write another article on the topic of breast shaping just to keep things separate.


