
Blame the Americans. Let me explain.
It is rather fascinating I think that the Americans have only had access to Motiva breast implants for about 6 months (compared to nearly 10 years in Australia) and they are flooding social medial with their apparent "expertise" in how to use them. I've seen some pretty remarkable (by which I mean totally incorrect) things written/said/posted by some plastic surgeons in the USA in the last few months. So, Motiva has taken plastic surgery in the USA by storm and has been plastered all across instagram in a way that simply never occurred here in Australia. We just haven't ever really seen Australian surgeons promoting themselves on the basis of the implants they use.
But of course, instagram (and indeed American advertising schtick) is always about the next big thing, so it seems we now have to move on from just using the Motiva implants to something else (to keep the eyeballs engaged), and anyone who has an even passing interest in plastic surgery, and almost certainly anyone who is researching breast augmentation or breast implants will have come across something called Preservé recently.
So, what the hell is Preservé, and why won't instragram shut up about it?
Now, there are a couple of really interesting points to consider here.
Firstly, as anyone in Australia is aware, we have some serious restrictions on what we can say and do as surgeons, especially when it comes to spruiking ourselves. Americans on the other hand: absolutely ANYTHING goes. They can literally make any sort of claim whilst making an absolute ass of themselves on Tik-Tok, and there seems to be nothing to stop them. So, Australian patients will have this kind of duality they are exposed to - the very "factual", rigid, and boring social media of Australian surgeons; and the unreal, bombastic (and sometimes totally full of shit) social media of our American brethren. That creates a curious juxtaposition.
Secondly (and again, as anyone in Australia is aware) surgeons here are deeply wedded to the idea of "dual-plane" breast augmentation. The Americans on the other hand...not so much. They have had a very long history of a far less rigid approach to how they do breast augmentation. There are probably reasons for that, but that is a whole different article.
And finally, I would offer the observation that Australian surgeons are curiously rigid, slow to change (terrified of change in some respects), and far more comfortable sitting with the status quo. Maybe that has to do with the classic Australian tall-poppy syndrome thing, I dunno - no one wants to stick out too far from the competition. The Americans, by contrast, will literally jump onto every new bandwagon, every new trend, and they absolutely love to have that "first-mover" advantage over their competition.
So, keeping all of that in mind, let's talk about Preservé.
Over the years, there have been several attempts to make breast augmentation procedures LESS invasive. Now, in the same way as "keyhole" or laparoscopic surgery is "less invasive" than a great big cut on the abdomen, what this really means is making the incision on the skin smaller, even though the extent of surgery performed inside is just as extensive, no matter the technique.
In a way, searching for less invasive breast surgery techniques has been more about marketing than about outcomes.
We've variously seen implants put in via the classic cut under the breast, around the areola (abandoned due to implant contamination issues and hence capsular contracture), through the armpit (using endoscopic instruments, developed during the 90's to avoid the "stigmatic" under-the-breast scar that had growing awareness in pop culture; abandoned due to implant malposition problems and contamination also), through the umbilicus (a bit of a niche idea, only possible with saline implants, and again with enoscopic instruments), and even via abdominoplasty incisions (and appalling idea, fortunately it never took off). All of those techniques apart from the inframammary incision have fallen away due to the progressive understanding of why the IMF incision is superior - better control of implant position, greater reduction of risk (of bleeding, of capsular contracture), and consequently greater durability of the outcome.
And over time, the IMF incision has gotten shorter. From something around 6-7cm 30 years ago, to the current claimed 2.5-3cm incision that some surgeons shout about obnoxiously on their reels. The shorter incisions have been made possible by changes in implant technology, and changes in delivery apparatus. The most recent change (in the last 15 years) is the use of funnels to deliver the implant after the pocket is made. This "no-touch" delivery device operates like a piping bag to squeeze an implant through a very small incision, but depends on the deforming characteristics of certain implant gels to avoid damaging the implant.
So, the current status quo is the development of a precise pocket (whether under or over the muscle) using diathermy (to ensure there is no bleeding), with careful pocket and implant washing (to minimise bacterial colonisation), and squeezing the implant in with a funnel (to allow a smaller cut and to prevent skin contact) followed by some sort of reinforcement of the breast crease with the closure (the fabled "internal bra" stitch...ugh).
And, let's be honest - that works pretty well for most surgeons, and many patients.
In terms of decreasing "invasiveness" though, there has also been a pretty strong swing (in the USA and South America particularly) away from dual-plane, toward over-the-muscle techniques (whether subfascial or not) due to patient preference for a more natural result that isn't plagued by animation deformity and the un-aesthetic consequences of sticking implants under Pec muscles. Now, that hasn't been picked up in Australia (for reasons I mentioned above, really), but regardless, this is an important consideration in what Preservé claims to offer.
So, that brings us to the question of how can breast augmentation be further refined to perform augmentation via limited incisions, with the least "invasiveness", but whilst preserving the control elements that allow for durable results?
Enter Dr Charles Randquist: interesting chap, bit too much botox, but (and let's be honest, this is cool AF) literally owns his own, private hospital in an incredible chateau on the waterfront in Stockholm like some kind of cosmetic Bond villain. Total baller. I'm a bit of a fan.
Dr Randquist (can we call him Charlie?) is not a new player. He was one of the early movers in the 90s (along with his colleague/mentor, Dr Per Heden who pioneered the so-called AK method of breast augmentation assessment that remains incredibly widely used) towards dual plane augmentation with anatomical breast implants. He really made his name in that space, and has been on the conference circuit as a speaker for a long time. But, interestingly it seems he was also quick to see the slow motion car crash of that approach and abandoned the near-religious dogma of dual-plane/anatomical implants (that so many Australian surgeons remain enraptured by) and started to think outside the box.
First, he made the early move in Europe to Motiva implants (who, like us have had access to Motiva for ages). In the last few years though, it seems that Charlie really got to work...and by that, I mean he jumped into bed with Motiva to try to develop a brand new set of techniques. I love an innovator, so let's look at what that collaboration has resulted in.
Dr Ranquist's efforts have resulted in two proprietary techniques (with associated instrumentation, and one presumes, healthy royalties): Preservé, and Mia Femtech (Mia is actually an acronym for "minimally invasive augmentation").
The basic idea that underlies both Preservé and Mia is that of "Tissue Preservation".
And this is the especially buzzy thing that is all over the place on socials. So-called "tissue preservation" is the latest sales pitch to ladies considering breast augmentation. This has certainly gone hand-in-hand with the trend towards smaller implants, more modest busts, and a desire for a natural (albeit enhanced) aesthetic.
"Tissue preservation" is just the latest in an endless litany of buzzwords in plastic surgery.
The basic premise of tissue preservation is that rather than cutting tissues to create a pocket into which an implant is placed, a space is created using what might be called "blunt" tissue spreading techniques. Again, this is a bit of an old-is-new-again concept - historically, breast augmentation was performed with a rather brutal, blunt technique using a large hockey-stick shaped device that was inserted and simply pushed around to create a pocket. That technique - which was used to create pockets under the muscle - was abandoned due to the risks of bleeding (which was associated also wtih higher risks of capsular contracture) and replaced with the more modern approach of using diathermy to create precise, careful pockets, and to control bleeding.
So what makes the "new" blunt dissection different to the "old" blunt dissection?
I think the first thing to say is that these new techniques are exclusively pre-pectoral. That is important. The risks of bleeding are certainly higher under the muscle. But more importantly, a pocket created under the muscle has a much greater tendency to expand due to the very flimsy tissue layer that exists between the ribs and the muscle. Which means that if this technique was used under the muscle, not only would bleeding again be an issue, but the control of the pocket would be poor at best.
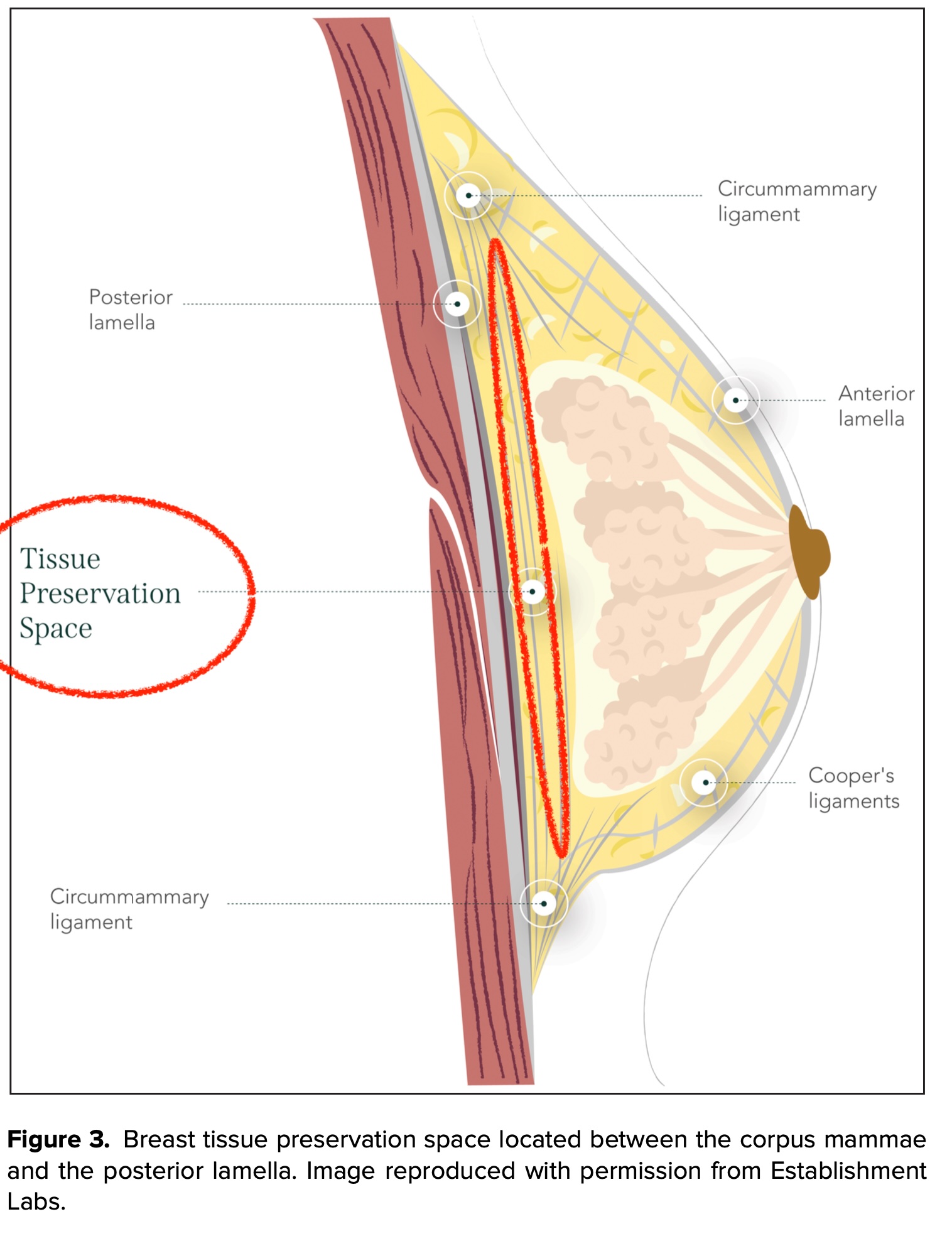
You can see in the image above that the intended position of the implant is not only over the muscle, it is also NOT under the Pectoralis fascia - that is, it ISN'T a subfascial technique. Which is probably good, because in my opinion, the whole subfascial thing is mostly confected rubbish when compared to a true subglandular approach - none of the evidence to support subfascial is compelling, and that is even more so when we consider modern implants.
The other thing that is new is the nature of the blunt dissection. Rather than a brute force, pushing approach to separate tissue layers (which is how we did it 25 years ago), both Preservé and Mia use an inflatable balloon dissector to create a precise space for the implant to sit in.
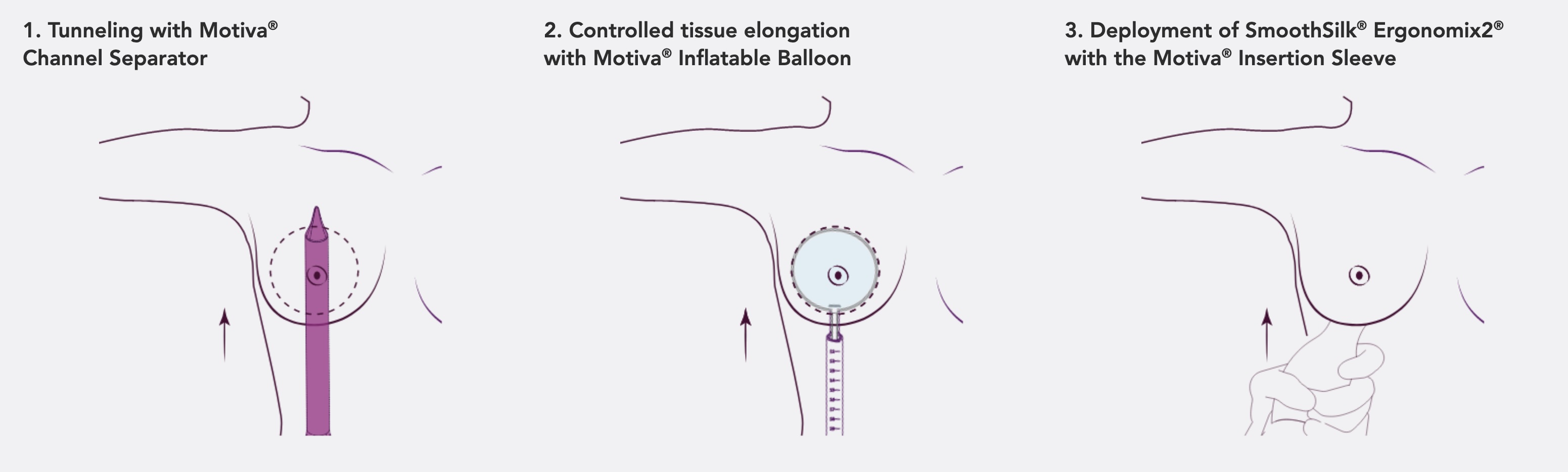
Essentially, both techniques boil down to the same thing: make a 2.5cm incision, use a pointy-ish plastic instrument that looks like an oversized knitting needle and shove that in using surface markings to indicate how far to go and in what direction (depending on the implant you want) to create a channel, then into that channel you push in a deflated balloon which is then inflated once in position to the size of the chosen implant, and then using special instruments the implants are squeezed into that space.
The idea is that by using a balloon to expand that space behind the breast gland (but in front of the fascia), the natural ligaments (the "circummammary ligament" forms a ring - sort of - around the breast and depending on the patient, is more or less defined) which surround the breast are preserved (hence, tissue preservation). The point of that is to maintain the natural structures which can support the implant, rather than cutting them in the traditional breast augmentation techniques and subsequently needing to reconstruct that support (with the so-called "internal bra" suture for example).
Couple of very important things to note at this stage:
Firstly, you can appreciate that with this technique, there is no ability to modify the breast itself - so if the breast shape or structure isn't right, this technique won't work.
Secondly, there are implant size limits by virtue of the way the dissection is done, the size of the incision and the reliance on natural supporting structures. What we're seeing with the early results of the Mia technique are implants that are very modest - between 140-200cc in most cases. The Preservé technique allows larger implants than the Mia (the access under the breast is more direct than via the armpit), and in some cases I've seen implants up around 350-400cc being placed, but I reckon anyone using over 300cc with these techniques might be looking at trouble.
Now, the very sensible people will be wondering about a few things here.
Let's think critically about this for a moment.
The biggest question to ask is WHY? Is Preservé just change for the sake of change, or is it genuinely going to lead to better outcomes?
Good question.
The answer is that we have no idea. The data is short term. The patients in whom these techniques have been used are carefully selected for studies. It is only with a combination of longer term data (to understand whether the results are durable etc), combined with the less controlled practices that we'll inevitably see once these techniques are released into the wild, that we'll be able to properly answer that.
For now, these "tissue preservation" techniques are interesting, but it might all be total bullshit too. For now, they are also exposed to worrying degrees of hype and marketing spin in the USA. The Americans are doing us a disservice here with their behaviour on social media, becuase what has happened is that the technique is becoming well known (to patients) without anyone being able to say that it is actually a good thing. I suspect that the more sensible surgeons out there are probably looking at this with a little skepticism...but in the cosmetic breast augmentation space, the need to keep up with the competition is going to create a demand/drive for people to take up this technique and because this is a technique that demands correct patient selection, I have no doubt we'll then see it applied in the wrong patients, leading to poor outcomes.
This will very likely mean that some of the early adopters will get shitty results...and instead of blaming themselves, they'll blame the technique. So techniques like Preservé then find themselves at risk of early uptake, followed by early abandonment if the people using it aren't properly trained and don't respect the limits of the technique. We've seen that many times before with different technologies, and one of the most obvious examples in recent times is with fat transfer systems - we saw people trying new fat processing techniques, getting bad results because they did a rubbish job, and then blaming the equipment rather than themselves.
Another question to ask is how many patients will this technique really suit? If there is no ability to modify the breast, doesn't that limit this technique to those ladies with essentially perfectly shaped breasts?
I am very sure that some of the early patients in whom Preservé or Mia are used (outside of studies) will end up with poor results because they weren't the right patient for the technique. Ladies with minor ptosis, mild tuberousness, anatomical differences...whatever the case, it seems to me that these tissue preservation techniques really demand patients with essentially perfectly shaped breast who just want a subtle enlargement. As soon as there is any requirement for trying to force the breast into a different shape, or any requirement to address the underlying footprint of the breast, we'll end up seeing problems. The potentially saving grace here is that the techniques are designed (ideally) for small implants - the smaller the implant, the more "forgiving" that can be for a surgeon. If you consider a ratio of implant:breast, the higher the implant value in that ratio (ie. massive implants:small native breast) the more likely you are to see problems crop up - things like double bubble, residual creases, bottoming out, malposition etc. So perhaps that will minimise some of the drama.
And what about this (relating to the Mia technique): why are we back to going through the armpit? That technique was largely discarded years ago for good reason, so what's changed?
I think that is a fair question but we can also look at how Mia differs to traditional endoscopic transaxillary breast augmentation to understand why we may not see the same problems.
The major issue with the transaxillary augmentations (the ones that I see for explant, anyway) is implant malposition (becuase of an inability to control the muscle in particular). Yes, there has also been a tendency to higher capsular contracture rates with insertion via the axilla, but that is something that I think can be mitigated with contemporary strategies like antibacterial washes and avoiding skin contact.
The major points that will make a difference here are going to be the prepectoral placement (which as I said above, will be less likely to suffer from malposition due to the muscle), and the fact that the Mia technique is really designed for very subtle implants under 200cc. This will be the technique that will facilitate the so-called "ballerina breast" or "fashion implants". These are some more (quite annoying) buzzwords that we are hearing a lot of on social media, which essentially refer to the very subtle, did-she-or-didn't-she (oh boy, I can't believe I just used such a horrible cliché, but whatever) kind of breast augmentation outcomes.
And finally, the thing that is really on my mind right now, is this: what are these damn things going to be like when we take 'em out? Will it be harder, easier, better, worse? I look forward to the inevitable explants coming my way from the first batch of Preservé augments in a few years time. Honestly! I'm curious.
One of the main criticisms I have of all breast augmentation techniques is that they don't account for their inevitable failure and requirement for implant removal. I've spoken about this a bit before and I will be interested to see what happens with these new techniques. I suspect that if the placement is accurate, it will actually make the removal relatively straightforward. However, the big challenge with any blind/blunt technique like Preservé is the risk of inadvertent placement in the wrong layer.
So, perhaps I should ask a different question: how many implants placed via the Preservé and Mia techniques will end in the wrong bloody spot? How many will end up accidentally in the Pec muscle?
The early studies have suggested using high-resolution ultrasound (like the kind we use in the rooms to assess implants for rupture) as a way of confirming placement. I think that is a good idea, but how many of the surgeons jumping on the bandwagon will actually do it?
Time will tell.
Final thoughts, for now:
I am interested to see innovation in the breast augmentation process. I think that, for way too long, breast augmentation has just been this lurking monolith of a procedure, with surgeons doing exactly the same thing as they've done since the '90s.
Will "tissue preservation" be a true revolution? I don't know. The data remains very early. And industry involvement is all over the studies we have available at this time.
To answer the question that some patients might then ask me: will Preservé or Mia be sufficient to convince me to start doing cosmetic breast augmentation? I doubt it. Of course, it will depend on the safety data and the longer term functional and cosmetic outcomes (and also the number of ladies I see for explant after Preservé). Right now, the trend towards smaller implants definitely will favour the uptake of tissue preservation techniques more generally though, but will those results be BETTER than current standard breast augmentation techniques? Let's reconvene on that question in 5-10 years!
I think the real application here is part of the increasing use of very small breast implants. What I find intriguing is the prospect of a surgical technique offering very subtle results in a way that might almost be considered analagous to what patients are seeking with fat transfer. The point of course being that this technique would be possible where fat transfer might not be (eg. in the very lean/slim patient). On that note, I will also try to write something soon also about the new "off the shelf" fat products (in particular, a product called Alloclae) that are now available in the USA (but not yet in Australia) becuase that might similarly be something of a game-changer...but we'll see. So keep an eye out for that.
Just to be clear, Motiva Preservé is NOT YET AVAILABLE IN AUSTRALIA. It will be launching in Australia in August 2026, in conjunction with the new Motiva Ergonimix 2 (which are softer than current Ergonomix implants) implants which already have their TGA approval as I understand it. The Femtech Mia system is not available in Australia either and probably won't be coming here. The Motiva Ergonomix "Diamond" implants (which are biconvex) required for the Mia system do not have any TGA approval, and nor does the Mia equipment.
The reason I say that is because I've seen a few folks trying to suggest that they are doing something similar (early movers trying to get the jump perhaps). There is, for example, a chap in Sydney who seems to have coined a cute little acronym for himself to suggest that he is doing a "balloon assisted" dissection of some description. To be honest, I have no idea what he's doing, but he definitely isn't using the Preservé system at this time.
I am sure that, for surgeons who do cosmetic breast augmentation, it's an exciting time. And with that will come a degree of risk for patients. Worth keeping in mind.


